Showing posts with label real. Show all posts
Showing posts with label real. Show all posts
Implementing Shared Decision Making In The Real World
Monday, May 12, 2014
.jpeg)
Except for the part about the DMCB, thats what basically happened at the eight highly regarded medical institutions: Dartmouth-Hitchcock Medical Center, MaineHealth, Massachusetts General Hospital, Mercy Clinics in Iowa, the Oregon Rural Practice–Based Research Network, the Palo Alto Medical Foundation, the Stillwater Medical Group in Minnesota and the University of North Carolina at Chapel Hill. The decision aids covered approximately 50 common conditions such as knee arthritis and prostate enlargement
And it didnt work out.
To investigate what happened, investigators at RAND interviewed 23 "key informants" from the 34 primary care sites that had implemented the Informed Medical Decision Foundations shared decision making program. The interviews were conducted between December 2010 and March 2011. Their study is published in the February issue of Health Affairs.
Three barriers were identified:
Overworked physicians: given all the other health care needs of their patients, it was difficult to count on physicians to distribute the decision aids. As a result, only 10%-30% of eligible patients participated.
Overconfident physicians: many doctors felt that they were already providing sufficient patient education or that their patients would not benefit from the decision aids. Just telling the docs that this worked was not enough.
Underperforming EHRs: the state-of-the-art information technology could not flag potential patents, remember which individuals had been exposed to the decision aids or record the patients perences.
The answers?
Well, if the someone from the eight institutions had simply called the DMCB and asked, it would have told them about the many times it explained stuff to a roomful of physicians and had zero impact. There also good peer-reviewed literature on why its so difficult to change physician behavior.
The DMCB ultimately found the answer is to take physicians out of the work flow.
Thats what the RAND researchers found. Based on their interviews, they recommend that if youre going to implement SDM in your clinics:
Automate the process as much as possible and remove human decision-making from the process the triggered the decision aid. That could be done on the basis of pre-existing clinical criteria or when a specialist erral had been arranged.
If automation was not feasible, rely on non-physicians to trigger the decision-aid. For example, office assistants could offer SDM to patients in the course of check-out.
Image from Wikipedia

Real Life Farmville 2013
Saturday, April 26, 2014
Its that time again, folks... Spring time is here! Warming weather, flowers blooming, happy people everywhere... But one of my favorite parts about the Spring is starting my vegetable garden. This will be my fourth year having a garden. Ive learned a lot from my mistakes over the past three years, and Im ready for this year to be the best yet! Anything worth doing is worth doing badly, thats what I always say. No one is good in the beginning, just do it. Just do something.
So Real-Life Farmville 2013 is underway, and Id like to share with you what Ive got going. Ive been buying my seeds from Seed Savers Exchange every year. Theyve got tons of unique, heirloom varieties of vegetables, and theyll send you an amazing catalog showing you everything they offer... highly recommended. I like trying different stuff since my uncle, who shares the garden with me, always grows the common veggies like cucumbers, tomatoes, and summer squash. Im a little more adventurous.
First up is the herbs... this is a new addition this year.
Got this little guy as an Easter gift in one of those easy-grow pots. It came with blocks of dry soil, all I had to do was add water and plant the seeds and watch it grow. Cant wait to use this stuff in my kitchen!
For the rest, I got 4 soil-filled flats from my family farm, Botticello Farms. Ive been putting them outside every day and taking them in every night to avoid the cold weather, and theyve been doing very well on that regimen. Its only been a week and a half and theyre looking good already!
Lets start with the kale, as this has been my most successful crop over the years.
Kale never fails. Thats what Ive learned. It always grows and its very resilient; it can be out in below-freezing temperatures, no problem. It will also grow all summer long and give you a constant supply of leaves. Good stuff.
Next up... this is my baby... a little yellow grape tomato called blondkopfchen.
Ive had these the past 3 years and Ive saved the seeds every year, so I take pride in these little guys. This is my third generation, and I just cant wait til mid-August when theyre ready to be picked. Theyre like red grape tomatoes, but with a little extra sweetness. Sweetness.
Next up Ive got some rainbow chard, a new one this year.
We did plain old Swiss chard last year, but I thought Id try a more colorful variety. Its looking strong so far. Cant wait to try these, chard is great in my morning omelets!
Next! An heirloom variety of tomatoes called Black Sea Man.
Ugly looking? Yes. But they look super delicious and yummy.
Then we have some onions.
These are Ailsa Craig onions, which is supposedly an heirloom variety, although they look pretty much just like normal yellow onions.
And finally weve got 3 different types of lettuce... Grandpa Admires, Rossa di Trento, and Oak Leaf.
This will be my first time trying to grow lettuce, and Ive got about 72 of these little guys so hopefully it works out! Ill be putting those in the ground very soon.
Welp, thats it for my garden this year. Super excited to be able to use this stuff in my kitchen, theres truly nothing like garden-fresh veggies!
Anybody out there starting a garden this year? Tell me all about it in the comments!
So Real-Life Farmville 2013 is underway, and Id like to share with you what Ive got going. Ive been buying my seeds from Seed Savers Exchange every year. Theyve got tons of unique, heirloom varieties of vegetables, and theyll send you an amazing catalog showing you everything they offer... highly recommended. I like trying different stuff since my uncle, who shares the garden with me, always grows the common veggies like cucumbers, tomatoes, and summer squash. Im a little more adventurous.
First up is the herbs... this is a new addition this year.
 |
| Herbs: Parsley, Cilantro, Dill |
Got this little guy as an Easter gift in one of those easy-grow pots. It came with blocks of dry soil, all I had to do was add water and plant the seeds and watch it grow. Cant wait to use this stuff in my kitchen!
For the rest, I got 4 soil-filled flats from my family farm, Botticello Farms. Ive been putting them outside every day and taking them in every night to avoid the cold weather, and theyve been doing very well on that regimen. Its only been a week and a half and theyre looking good already!
Lets start with the kale, as this has been my most successful crop over the years.
 |
| Now |
 |
| Later |
Next up... this is my baby... a little yellow grape tomato called blondkopfchen.
 |
| Now |
 |
| Later |
Ive had these the past 3 years and Ive saved the seeds every year, so I take pride in these little guys. This is my third generation, and I just cant wait til mid-August when theyre ready to be picked. Theyre like red grape tomatoes, but with a little extra sweetness. Sweetness.
Next up Ive got some rainbow chard, a new one this year.
 |
| Now |
 |
| Later |
We did plain old Swiss chard last year, but I thought Id try a more colorful variety. Its looking strong so far. Cant wait to try these, chard is great in my morning omelets!
Next! An heirloom variety of tomatoes called Black Sea Man.
 |
| Now |
 |
| Later |
Then we have some onions.
 |
| Now |
 |
| Later |
And finally weve got 3 different types of lettuce... Grandpa Admires, Rossa di Trento, and Oak Leaf.
 |
| Now. They all look the same at this point. |
 |
| Later. Grandpas. |
 |
| Later. Oak Leaf. |
 |
| Later. Rossa. |
Welp, thats it for my garden this year. Super excited to be able to use this stuff in my kitchen, theres truly nothing like garden-fresh veggies!
Anybody out there starting a garden this year? Tell me all about it in the comments!
The Real Business Model For Virtual Medical Office Visits and its not increasing access
Friday, February 28, 2014
 |
| "Stand up, bend over and let me see that itchy rash!" |
It worked pretty well. Whats more, the literature suggests that this is not all that new, there are studies that suggest high levels of patient satisfaction and a surprising willingness to pay for the service out of pocket. Time will tell on whether this leads to comparable clinical outcomes at an acceptable cost.
But what has struck the DMCB most of all was a business model "dichotomy." Talk to most policymakers about virtual office visits and youll discover that it is being hailed as another advance in increasing consumer-patient access to cost-effective care. In other words, persons living in Faraway Montana will be able to discuss their rash with the expert Dr. Windowchat anywhere in the world. The DMCB thinks of this as the "enlightened" side of "telemedicine."
While that may have merit, when the DMCB googles "virtual office visits," it finds a decidedly contrary business model: busy and computer-savvy suburbanites with the kind of disposable income who can pay out-of-pocket for the convenience of not having to sit in a waiting room. From a health insurance perspective, this is quite compelling, since it substitutes a lower level of service for a population that is prone to overutilization. The DMCB knows the doctors like it better when the insurers arent involved in a high cash-flow yes-Ill-take-VISA transactional business. This is the "real" side of telemedicine.
The DMCB suspects this is one of those innovations that offers something for everyone: increased access for those with not enough of it and "disruptive" technology for a health care industry still locked into expensive and labor intensive one-on-one doctor-patient visits. From all points of view, this form of telemedicines future is very bright.
Real News Headline Improved U S Health Care System Saves 28 000 Lives in 2010 Avoidable Death Rate is Decreasing
Sunday, February 9, 2014
.jpg) |
| Health reporters at work |
The information reported in the media was taken from the Centers for Disease Control and Preventions Sept. 3 Morbidity and Mortality Weekly Report. As the DMCB understands it, the CDC authors pulled 2001-2010 mortality data from the National Vital Statistics System. Once that was done, they counted up the number of persons aged less than 75 years who died of "ischemic heart disease," "cerebrovascular disease," hypertensive disease" or "chronic rheumatic heart disease."
So what did MMWR really say?
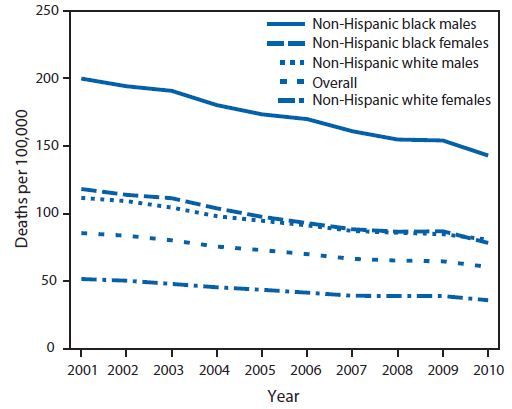
The total of "less-than-75" deaths in 2001 was 227,961. For 2010, it was lower at 200,070. Since the population in the U.S. has changed over the last decade, the totals for each of the two comparison years were then expressed as a "per 100,000" statistic.
Since 2001, the "less-than-75" death rate per 100,000 declined by 29%. The decline averaged 3.8% a year.* Persons age 65-74 years had an average decline of 5.1% vs. 3.3% persons between the ages of 55-64.
The good news is that Black (3.9%) and Hispanic (4.5%) persons had greater declines than whites (3.6%). The bad news is that they started and ended with a higher death rate.
Heres a visual display of the data:
The DMCBs take
1. "Avoidable?" The CDC definition implies that perfect control of all cardiac risk factors (for example, cholesterol and weight) for everyone under the age of 75 will result in a 0 per 100,000 cardiovascular death rate. Not so, because those risk classic factors capture some, but not all, persons who succumb to heart attack and stroke.
2. So, this is bad news? "200,000" deaths is an impressive number, but, on an unadjusted basis, thats about 28,000 fewer compared to 10 years ago. Some additional good news is that the U.S. rate of non-fatal heart attack and stroke appears to have dropped significantly also. We are making significant headway in the battle against heart disease.
3. The real story? Persons of color have had the greatest relative benefit but still have the greatest absolute need. That lingering health care disparity went shamefully unmentioned by CNN and was only briefly mentioned by USAToday.
4. Something for everyone: In their "Conclusions and Comments," the authors of the MMWR paper speculated on the benefits of the (still unproven) Million Hearts Initiative (a Berwick-era idea) as well as "health information technology" and various "community prevention strategies" The DMCBs colleagues in the care management service industry will really like the authors nods toward "team based care" and how "individuals can work toward reducing their own heart disease and stroke risk." If the CDC says so, it must be true - assuming theres a good business model.
5. Speaking of speculation, the authors wondered if the greater decline in the Medicare age group (65-74 years) versus the younger age group (55-64) was because of the presence of health insurance. Maybe, but maybe not. The DMCB also wonders if heart disease is more lethal and less amenable to intervention among younger persons, but cant find any literature to back that up.
6. Politics intrude: Naturally, the scientists who write MMWR are too classy than to curry favor with the appointees that populate the upper echelons of the federal bureaucracy, but that didnt stop the CDC Vital Signs from shamefully putting in a "making it easier for Americans to afford regular preventive health care through the Affordable Care Act" plug. The ACA was not mentioned in the MMWR report because the declines mentioned above occurred in the absence of the ACA.
The DMCB predicts that when the "avoidable" death rate continues to decline by 3.8% in the coming years, Obamacare advocates will take the credit.
*The DMCB isnt sure how 3.8% for 10 years makes for 29% either, but thats statistics for you.
Image from Wikipedia
The Real Cause of Cardiovascular Disease And The Benefits of Chelation Therapy
I have spent over 35 years researching chelation therapy (CT), trying to determine how and why it helps patients with cardiovascular disease (CVD). I strongly believe that some form of CT should be a part of the treatment for anyone with CVD. My knowledge of CT has permitted me to safely advise against all bypass operations on my patients for over 30 years.
I knew that this was working, but I jumped to the wrong conclusion: I thought that somehow CT must be reversing plaque, never dreaming that removing heavy metals could bring these benefits. My error probably set back the widespread acceptance of CT by decades, as knowledgeable invasive cardiologists often found that serious "obstructing" plaque was still present after CT.
I have since identified over 30 mechanisms of action of EDTA. Any one or all of these working synergistically can explain why over 80% of patients get both subjective and objective improvement. However, it is still not possible to predict when sometimes more-dramatic benefits will occur, including occasional rapid saving of gangrenous legs, reversal of heart disease or blindness, or the occasional autistic child who within hours recovers speech. Since we have poisoned our planet, I believe that heavy metal detoxification is a big part of the explanation for the benefits seen, even in nonexposed patients. All causes of morbidity and mortality have been shown to relate to how low lead levels are kept throughout life.
There is no magic program that can remove all of our heavy metals or other toxins overnight. We need several years to decrease the body burden of lead, as bones will remodel over a period of 15 years. I recommend continuous use of one or more aids to detoxification such as chelators, high-dose vitamin C, fiber, lipoic acid, zeolite, saunas, and daily exercise. These all provide benefits that greatly exceed any risks involved. For example, the various claims about chelation toxicity, such as harming the kidneys, although possible, are greatly exaggerated. In fact, repeated EDTA infusions often postpone indefinitely the need to start dialysis for many patients in early renal failure.
Due to my own CVD, I have intensively studied all aspects of it for most of the 50-plus years of medical practice. I have a complex medical history with lifelong heart disease issues that by age 29 had become nearly disabling; I avoided most physical activities until I was well in my 30s. When I first chelated, it was with with great results: hours after my eighth intravenous EDTA treatment, I felt like Superman! I could for the first time in my life run uphill without a racing heart, or chest pain, or fatigue.
I have acquired and reviewed thousands of articles and books about chelation and heavy metals; I have treated hundreds of patients, and seen many dramatic responses, yet I warn my patients that CT does not predictably by itself decrease plaque. However, improved blood flow happens in over 80% of patients. With more treatment and improved compliance with my "FIGHT" Program (Food, Infection, Genetics, Heavy metals/Hormones, Toxins), over 95% will improve, even if the angiograms report that plaque size has increased. This experience and my radiology training confirm the limitation of angiograms, which fail to identify the existence of collateral circulation, as seen with a PET scan.
Obstructing plaque or vascular calcium scores may appear worse after CT, yet the patient has dramatic subjective and objective improvement, and is now winning in competitive sports. I per noninvasive tests that more accurately assess the true status. They are useful and can motivate patients to try harder, as a poor response may just be a patients failing to address all risk factors
In my own case, I had a mouthful of amalgam fillings, and part of my dramatic early response was due to removing heavy metals, which we now know interfere with healthy enzyme function and thus impair nitric oxide levels. Improved nitric oxide function is another reason for the predictable improvement in blood flow seen with all noninvasive measurements, including segmental blood pressures, thermography, plethesmography, Bio Clip, and multifunction ECG.
Researchers at California Institute of Technology have shown that average bone lead levels today are 1000 times higher than a few hundred years ago. Studies at Harvard have shown that higher bone lead contributes to cataract formation and 6 times more heart attacks. I conclude from my 35-year review of literature and worldwide attendance at environmental, anti-aging, ACAM (American College for Advancement in Medicine), and related conferences that we cannot reach our maximum intended useful lifespan or enjoy truly optimal health unless we are continuously detoxing.
Soft tissue lead stores are readily mobilizable, whereas bone lead is not, since bones take 15 years to remodel. While detoxing bones, we are still breathing in heavy metals as particulate matter from coal-burning for power, as well as taking in lead every day from our water, food, and air. This has made safe, convenient oral detoxification daily for life so essential today.
Frequent consumption of fish leads to mercury toxicity, and lead makes mercury more toxic, so we develop symptoms that are not cured by drugs. Genetics is involved, whereby some people after eating fish excrete mercury efficiently in 40 days, while others require 140 days.
There is no simple solution that meets all our detoxification needs, as we must deal also with organics. Some newer forms of zeolite work well for mercury, as well as for some organic toxins. I recommend regular use of one or more of the following detox measures: parenteral or oral EDTA, DMSA, DMPS, zeolite, greens, maca, garlic, vitamin C, fiber (as stabilized rice bran or modified citrus pectin), NAC, lipoic acid, exercise, sweating, saunas, and organic foods.
Dr. Rodger L. Bick, as a world expert on thrombosis, stated that blood clots kill over 3 million in the US alone each year, but are usually just called heart attacks or strokes, which occur when the vulnerable plaque ruptures.
My patients are shown a five-minute video of a vulnerable plaque breaking open and exposing subintimal tissues, which leads to the formation of a fatal blood clot. This graphic helps them understand that their supplement program is essential for life. Noninvasive vascular tests such as a new vascular age test, the Bio Clip, and the new multifunction EKG that is better than angiograms permit patients to see improvement and help me fine-tune the program when improvement is not adequate.
I rely on the textbook The Vulnerable Atherosclerotic Plaque for what I think is the best explanation of how and why death occurs from heart disease. (It took the American Heart Association many years to publish this.) I use this text, plus my professional experience and knowledge, to challenge most of the current dogma regarding the etiology and treatment of CVD. As a result, I routinely advise against all invasive procedures including angiograms, stents, and bypass surgery, as my program has a better risk-benefit ratio.
I explain the basic heart support program I use for patients in "The End of Heart Attacks Is in Sight," a guest chapter for Tony ODonnells latest book. Lester Morrison, MD, PhD, developed this approach to heart disease after he concluded that cholesterol was not the primary problem. Blood clots kill and heparin prevents clots, so he set out to develop a safe alternative to Coumadin and heparin. He spent $10 million doing the research that led to his nutritional program that modifies viscosity and clotting. He found a combination of several nutrients that act synergistically with his special mucopolysaccarides to help reverse arteriosclerosis and stop heart attacks.
Dr. Morrisons two published studies reported an average 91% reduction in fatal heart attacks using his institute formula. The addition of EDTA made it far more effective and led to its incorporation into oral packets of nine pills. These packets include a strong multivitamin, a capsule each of omega-3 and primrose oil, a phosphatidyl serine with Gingko biloba, and three capsules containing the EDTA-enhanced institute formula. This combination has been shown to lower viscosity using rheological testing. This is one reason that the packets help prevent fatal blood clots. Due to its weak benefits and side effects, I per these nine pills to aspirin, which I usually discontinue.
EDTA does much more than lower the body burden of toxic metals. The Morrison Institute Formula helps prevent clots, and EDTA enhances its anticoagulant effects. I focus on lowering blood viscosity and hypercoagulability, partly by lowering inflammation through diet and lowering total body burden of pathogens with oral advanced silver or other oxidative therapies.
In the years since Dr. Morrisons research was done, other nutrients such as vitamin D, resveratrol, vitamin K2 have become recognized and may now be part of the oral chelation packets. I have found that the nine-pill packets taken twice a day have virtually eliminated all fatal heart attacks and/or strokes in my patients for over 20 years now.
Ideally, most patients would also benefit from many other nutrients, such as CoQ10, carnitine, lipoic acid, acidophilus, and NAC; but due to cost, these are optional and taken separately along with other nutrients used by metabolic cardiologists.
Also, based on history or prior blood clot and/or lab tests results (for example with Leiden 5), I will recommend adding additional natural enzyme-based anticoagulant protection such as nattokinase, Wobenzym, or perably lumbrokinase(Boluoke).
Intracellular magnesium levels are relatively deficient in most chronic illnesses, partly because inflammation leads to increased intracellular calcium, which results in a relative magnesium deficiency. I often recommend the use of a series of weekly IV Myers cocktails, initially to provide magnesium and B vitamins, since even aggressive oral magnesium supplementation fails for a while, as it is poorly absorbed.
Lowering lead levels benefits almost anyone. Doctors Data found that calcium EDTA removes more lead than disodium EDTA per infusion. Thus I recommend a short series of IV calcium EDTA, which is painless, so it is often administered by chelation doctors over a 5- to 10-minute infusion time in place of the standard 3-hour infusion of disodium EDTA. Calcium EDTA may be given alone or as a mini-infusion with Myers or separately, one after the other directly from a syringe.
On my website forum, FACT (Forum on Anti-aging and Chelation Therapy), members report that they like this approach to chelation, as the results are comparable or even better and the process no longer ties up a room for hours. Patients like it since they do not lose a days work and will come in weekly for a time, and then monthly. This provides an opportunity to check their vitals, review their supplement programs, and reinforce the need to follow the total FIGHT Program.
I wrote the original protocol for the safe use of IV chelation 37 year ago, which was subsequently officially adopted by ACAM. Since then millions have been safely treated. Now with our improved understanding of the risk factors and the multifactorial aspects of CVD, I use the acronym FIGHT. I direct patients to my website (www.gordonresearch.com) to learn more and watch webinars on each of those topics. I also record every consultation and e-mail the digital copy to them so that they can review all of my recommendations anytime. That protects everyone: since I am routinely advising against bypass surgery, statins, and Coumadin, they have the recording, which explains why I believe that the benefit-to-risk ratio is better with my program, as it has proven extremely effective in showing low morbidity and mortality for over 20 years.
Since infection/inflammation is always involved in CVD, I often recommend a course with a well-documented advanced silver product that safely lowers the total body burden of all pathogens including cytomegalovirus, Coxsackie, Chlamydia, Candida, and Lyme. Also I routinely recommend 8 to 12 g of a high-dose, well-tolerated, powdered vitamin C delivery system that includes nutrients for methylation support. I also use sublingual B12 along with 5-MTHF.
If vascular testing shows high calcium scores, I recommend therapeutic levels of K2 to help reverse vascular calcification. This also requires stopping bone loss, so I add exercise, vitamin D, and a safe natural alternative to bioidentical hormone therapy: HRT Plus, a SERM (selective estrogen receptor modulator) beta from Thailand that also has proven anticancer effects, so it is safe for lifetime use. I explain how long-term management of CVD requires preventing calcium accumulation in arteries and that maintaining strong bones helps decrease vascular calcification and leads to soft, flexible arteries. High-dose calcium supplements alone are not the answer, since by age 80 the average person has 140 times too much calcium in his aorta.
I have attended hundreds of conferences hoping to improve my CV health and that of my patients. I share my information freely, as do the over 2300 health-professional members of FACT. Members can search any topic, such as the use of calcium EDTA or alternatives to Coumadin, and retrieve the latest information from the ever-growing shared database. Also if necessary, members may get a free "curbside consultation" about a patient or an issue, but only after you have exhausted your own review so that questions are not repetitive. I hope that you will visit the FACT forum website at http://promed.gordonresearch.com/factforum/index.php, and register and join us. I believe that you will find your practice becomes exciting and fun again.
I knew that this was working, but I jumped to the wrong conclusion: I thought that somehow CT must be reversing plaque, never dreaming that removing heavy metals could bring these benefits. My error probably set back the widespread acceptance of CT by decades, as knowledgeable invasive cardiologists often found that serious "obstructing" plaque was still present after CT.
I have since identified over 30 mechanisms of action of EDTA. Any one or all of these working synergistically can explain why over 80% of patients get both subjective and objective improvement. However, it is still not possible to predict when sometimes more-dramatic benefits will occur, including occasional rapid saving of gangrenous legs, reversal of heart disease or blindness, or the occasional autistic child who within hours recovers speech. Since we have poisoned our planet, I believe that heavy metal detoxification is a big part of the explanation for the benefits seen, even in nonexposed patients. All causes of morbidity and mortality have been shown to relate to how low lead levels are kept throughout life.
There is no magic program that can remove all of our heavy metals or other toxins overnight. We need several years to decrease the body burden of lead, as bones will remodel over a period of 15 years. I recommend continuous use of one or more aids to detoxification such as chelators, high-dose vitamin C, fiber, lipoic acid, zeolite, saunas, and daily exercise. These all provide benefits that greatly exceed any risks involved. For example, the various claims about chelation toxicity, such as harming the kidneys, although possible, are greatly exaggerated. In fact, repeated EDTA infusions often postpone indefinitely the need to start dialysis for many patients in early renal failure.
Due to my own CVD, I have intensively studied all aspects of it for most of the 50-plus years of medical practice. I have a complex medical history with lifelong heart disease issues that by age 29 had become nearly disabling; I avoided most physical activities until I was well in my 30s. When I first chelated, it was with with great results: hours after my eighth intravenous EDTA treatment, I felt like Superman! I could for the first time in my life run uphill without a racing heart, or chest pain, or fatigue.
I have acquired and reviewed thousands of articles and books about chelation and heavy metals; I have treated hundreds of patients, and seen many dramatic responses, yet I warn my patients that CT does not predictably by itself decrease plaque. However, improved blood flow happens in over 80% of patients. With more treatment and improved compliance with my "FIGHT" Program (Food, Infection, Genetics, Heavy metals/Hormones, Toxins), over 95% will improve, even if the angiograms report that plaque size has increased. This experience and my radiology training confirm the limitation of angiograms, which fail to identify the existence of collateral circulation, as seen with a PET scan.
Obstructing plaque or vascular calcium scores may appear worse after CT, yet the patient has dramatic subjective and objective improvement, and is now winning in competitive sports. I per noninvasive tests that more accurately assess the true status. They are useful and can motivate patients to try harder, as a poor response may just be a patients failing to address all risk factors
In my own case, I had a mouthful of amalgam fillings, and part of my dramatic early response was due to removing heavy metals, which we now know interfere with healthy enzyme function and thus impair nitric oxide levels. Improved nitric oxide function is another reason for the predictable improvement in blood flow seen with all noninvasive measurements, including segmental blood pressures, thermography, plethesmography, Bio Clip, and multifunction ECG.
Researchers at California Institute of Technology have shown that average bone lead levels today are 1000 times higher than a few hundred years ago. Studies at Harvard have shown that higher bone lead contributes to cataract formation and 6 times more heart attacks. I conclude from my 35-year review of literature and worldwide attendance at environmental, anti-aging, ACAM (American College for Advancement in Medicine), and related conferences that we cannot reach our maximum intended useful lifespan or enjoy truly optimal health unless we are continuously detoxing.
Soft tissue lead stores are readily mobilizable, whereas bone lead is not, since bones take 15 years to remodel. While detoxing bones, we are still breathing in heavy metals as particulate matter from coal-burning for power, as well as taking in lead every day from our water, food, and air. This has made safe, convenient oral detoxification daily for life so essential today.
Frequent consumption of fish leads to mercury toxicity, and lead makes mercury more toxic, so we develop symptoms that are not cured by drugs. Genetics is involved, whereby some people after eating fish excrete mercury efficiently in 40 days, while others require 140 days.
There is no simple solution that meets all our detoxification needs, as we must deal also with organics. Some newer forms of zeolite work well for mercury, as well as for some organic toxins. I recommend regular use of one or more of the following detox measures: parenteral or oral EDTA, DMSA, DMPS, zeolite, greens, maca, garlic, vitamin C, fiber (as stabilized rice bran or modified citrus pectin), NAC, lipoic acid, exercise, sweating, saunas, and organic foods.
Dr. Rodger L. Bick, as a world expert on thrombosis, stated that blood clots kill over 3 million in the US alone each year, but are usually just called heart attacks or strokes, which occur when the vulnerable plaque ruptures.
My patients are shown a five-minute video of a vulnerable plaque breaking open and exposing subintimal tissues, which leads to the formation of a fatal blood clot. This graphic helps them understand that their supplement program is essential for life. Noninvasive vascular tests such as a new vascular age test, the Bio Clip, and the new multifunction EKG that is better than angiograms permit patients to see improvement and help me fine-tune the program when improvement is not adequate.
I rely on the textbook The Vulnerable Atherosclerotic Plaque for what I think is the best explanation of how and why death occurs from heart disease. (It took the American Heart Association many years to publish this.) I use this text, plus my professional experience and knowledge, to challenge most of the current dogma regarding the etiology and treatment of CVD. As a result, I routinely advise against all invasive procedures including angiograms, stents, and bypass surgery, as my program has a better risk-benefit ratio.
I explain the basic heart support program I use for patients in "The End of Heart Attacks Is in Sight," a guest chapter for Tony ODonnells latest book. Lester Morrison, MD, PhD, developed this approach to heart disease after he concluded that cholesterol was not the primary problem. Blood clots kill and heparin prevents clots, so he set out to develop a safe alternative to Coumadin and heparin. He spent $10 million doing the research that led to his nutritional program that modifies viscosity and clotting. He found a combination of several nutrients that act synergistically with his special mucopolysaccarides to help reverse arteriosclerosis and stop heart attacks.
Dr. Morrisons two published studies reported an average 91% reduction in fatal heart attacks using his institute formula. The addition of EDTA made it far more effective and led to its incorporation into oral packets of nine pills. These packets include a strong multivitamin, a capsule each of omega-3 and primrose oil, a phosphatidyl serine with Gingko biloba, and three capsules containing the EDTA-enhanced institute formula. This combination has been shown to lower viscosity using rheological testing. This is one reason that the packets help prevent fatal blood clots. Due to its weak benefits and side effects, I per these nine pills to aspirin, which I usually discontinue.
EDTA does much more than lower the body burden of toxic metals. The Morrison Institute Formula helps prevent clots, and EDTA enhances its anticoagulant effects. I focus on lowering blood viscosity and hypercoagulability, partly by lowering inflammation through diet and lowering total body burden of pathogens with oral advanced silver or other oxidative therapies.
In the years since Dr. Morrisons research was done, other nutrients such as vitamin D, resveratrol, vitamin K2 have become recognized and may now be part of the oral chelation packets. I have found that the nine-pill packets taken twice a day have virtually eliminated all fatal heart attacks and/or strokes in my patients for over 20 years now.
Ideally, most patients would also benefit from many other nutrients, such as CoQ10, carnitine, lipoic acid, acidophilus, and NAC; but due to cost, these are optional and taken separately along with other nutrients used by metabolic cardiologists.
Also, based on history or prior blood clot and/or lab tests results (for example with Leiden 5), I will recommend adding additional natural enzyme-based anticoagulant protection such as nattokinase, Wobenzym, or perably lumbrokinase(Boluoke).
Intracellular magnesium levels are relatively deficient in most chronic illnesses, partly because inflammation leads to increased intracellular calcium, which results in a relative magnesium deficiency. I often recommend the use of a series of weekly IV Myers cocktails, initially to provide magnesium and B vitamins, since even aggressive oral magnesium supplementation fails for a while, as it is poorly absorbed.
Lowering lead levels benefits almost anyone. Doctors Data found that calcium EDTA removes more lead than disodium EDTA per infusion. Thus I recommend a short series of IV calcium EDTA, which is painless, so it is often administered by chelation doctors over a 5- to 10-minute infusion time in place of the standard 3-hour infusion of disodium EDTA. Calcium EDTA may be given alone or as a mini-infusion with Myers or separately, one after the other directly from a syringe.
On my website forum, FACT (Forum on Anti-aging and Chelation Therapy), members report that they like this approach to chelation, as the results are comparable or even better and the process no longer ties up a room for hours. Patients like it since they do not lose a days work and will come in weekly for a time, and then monthly. This provides an opportunity to check their vitals, review their supplement programs, and reinforce the need to follow the total FIGHT Program.
I wrote the original protocol for the safe use of IV chelation 37 year ago, which was subsequently officially adopted by ACAM. Since then millions have been safely treated. Now with our improved understanding of the risk factors and the multifactorial aspects of CVD, I use the acronym FIGHT. I direct patients to my website (www.gordonresearch.com) to learn more and watch webinars on each of those topics. I also record every consultation and e-mail the digital copy to them so that they can review all of my recommendations anytime. That protects everyone: since I am routinely advising against bypass surgery, statins, and Coumadin, they have the recording, which explains why I believe that the benefit-to-risk ratio is better with my program, as it has proven extremely effective in showing low morbidity and mortality for over 20 years.
Since infection/inflammation is always involved in CVD, I often recommend a course with a well-documented advanced silver product that safely lowers the total body burden of all pathogens including cytomegalovirus, Coxsackie, Chlamydia, Candida, and Lyme. Also I routinely recommend 8 to 12 g of a high-dose, well-tolerated, powdered vitamin C delivery system that includes nutrients for methylation support. I also use sublingual B12 along with 5-MTHF.
If vascular testing shows high calcium scores, I recommend therapeutic levels of K2 to help reverse vascular calcification. This also requires stopping bone loss, so I add exercise, vitamin D, and a safe natural alternative to bioidentical hormone therapy: HRT Plus, a SERM (selective estrogen receptor modulator) beta from Thailand that also has proven anticancer effects, so it is safe for lifetime use. I explain how long-term management of CVD requires preventing calcium accumulation in arteries and that maintaining strong bones helps decrease vascular calcification and leads to soft, flexible arteries. High-dose calcium supplements alone are not the answer, since by age 80 the average person has 140 times too much calcium in his aorta.
I have attended hundreds of conferences hoping to improve my CV health and that of my patients. I share my information freely, as do the over 2300 health-professional members of FACT. Members can search any topic, such as the use of calcium EDTA or alternatives to Coumadin, and retrieve the latest information from the ever-growing shared database. Also if necessary, members may get a free "curbside consultation" about a patient or an issue, but only after you have exhausted your own review so that questions are not repetitive. I hope that you will visit the FACT forum website at http://promed.gordonresearch.com/factforum/index.php, and register and join us. I believe that you will find your practice becomes exciting and fun again.
Eat Real Food
Saturday, February 8, 2014
Hi,
I just got back from visiting a friend who had been in a car accident last Wednesday. She called and told me about it on Saturday and hearing about it felt so shocking to me. I am so glad she was not injured more than she has had to deal with. Her leg is hurting her and her neck and shoulders, too. I took a little food and she and her two grand daughters and I had dinner together and talked and shared. I am so grateful to God that He spared her life this time. It really shows you just how precious life is and that we have only been granted so much time on Earth. That being true, puts things into a whole different perspective. God, family, and friends become so much more important.
I have been listening to "The Great Health Debate" which was eight days of one-hour health interviews of at least 16 different healthy living teachers covering the spectrum from vegan, meaning eating no meat or animal products of any kind, to the polar opposite which is those who eat meat for health. Wow. I have got to tell you this was really amazing to me to listen to such informed people and to find out why they do what they do. The most important thing to come from it all is this: what am I going to do with this information? We are all in that boat. What are you going to do in your life with the information you have.
Sean Croxton ( www.undergroundwellness.com ) one of todays experts said: "We are all different. We have something called biochemical individuality. The thing that works for me, may not work for the next person. Just eat real food. What I teach people is to listen to their body "language." Do what works for you." He also said, again, "Just eat real foods. Just eat foods that came out of the ground, eat foods that came (from) animals. Get rid of all the processed junk. Get rid of all the "new" foods. Be very wary of grains and legumes, and dairy products as well -- for a lot of people -- because of what they may do to the gut and the anti-nutrient properties that they can have. I try to keep it really simple for people so I tell them to eat real food." He also described going with the starting place of half of your plate animal food and the other half primarily vegetables. Once you try that then make the adjustments that your body tells you to make.
He talked about keeping it old school -- eating the same meat, fish, vegetables that we have eaten forever. He said that he does not believe that an old food will cause a new disease. Makes sense to me. He talked about our human genes having been around for thousands and thousands of years and there is food out there that has not been around for even twenty years. Shy away from that stuff. Keep it simple (without a lot of sauces and exotic concoctions). Keep it real (actual food, not chemically altered). Get rid of the processed food (manufactured food stuff) and eat real food. I am still going to cook my meat but the veggies should be raw. And I would add for us diabetics to get rid of all sugars. You can get along without them. High blood sugar comes from eating sugar and things that turn into sugar in the gut (grains, starchy foods, starchy vegetables).
Sean also quoted this statement: "Anything worth doing is worth doing poorly at first." It is an odd statement but there is some truth in it. I chuckled when he said it because I felt like I knew exactly what he was talking about. You cannot change your whole diet and be successful in just one day, it takes practice, it takes trial and error -- and if you are willing to start off doing it poorly, then you will continue until you do it better -- or you find a better way to do it. Who knows, one day you could end up being an "expert" but no one starts out there. Sometimes people are not willing to do things poorly, but in reality that is where every one is when you start. No one is perfect, even when they get to be experts, there is always something to work on.
After listening this week to the debate airings I am feeling relieved. I had been feeling down and discouraged because I just do not seem to be able to stick to a vegan diet, which I had felt was the right thing to do for my health. I felt that my "giving in" and starting to eat meat again was somehow a failure on my part, but the truth is, to fail means to quit and I have not quit, I am just continually making adjustments. I have had to change my mind and approach often, to keep up with the reality of my own life. Who is to say that being a vegan is the right thing for me to do? It works for some, but it surely wont work if you cannot stay on it.
I think it all boils down to mindful eating which Mike Adams ( http://www.naturalnews.com/index.html ) talked about. He talked about simply paying attention to what you are eating and thinking about it. He pointed out that most American and Europeans eat "mindlessly" -- using that word as a technical term meaning eating without thinking about what you are eating.
I know for myself, when I am eating things that I want to eat but know will harm my body in some way I have to turn off what my mind is saying about it. That is mindless eating. That is responding to feelings of some kind without responding to health or consequences.
For me, mindful eating would be choosing lots of fresh raw vegetables and also choosing healthy meat to eat. The thing is... that is what the Lord told me a long time ago. I have known that is the best solution for me all along, but, if not for the "30 Day Diabetes Cure" by Dr Ripich and Jim Healthy, I would not have started the journey to get close to my own ideal.
I know that I need to stay away from all sugars, including artificial or "new" sugars, like xylitol. It was trial and error that revealed the problems for my body with eating xylitol. I tried it. I erred. I corrected. I no longer eat that. I know that I should avoid all grains, too, but what I actually do is limit them. I do eat some food, occasionally, that is made from grain or flour. The ideal is "never" -- the practical ideal is "rarely." But even that is not where I live. Where I have a problem is with this "mindless" eating thing. Eating as if I have no mind. Purposefully making wrong choices for myself.... out of habit.... out of desire... out of some compulsion that I have. I would love to learn how to conquer that!!
This is a personal journey of discovery. As I was assembling my trash for disposal today the empty cracker boxes from last Wednesday when I bought some "healthy" crackers and ate them with either cottage cheese or avocado dip came rushing back into my consciousness. I also remembered the stomach cramps I got after having eaten them. The empty pizza box from Sat night slapped my face with remembrance, too. It is the mindless eating that I want to conquer. Looking for a solution to that.
I have noticed something about the mindless eating episodes that I had not noticed before. When I am doing that, there is a pressure inside of me. The last couple of times I did that, I noticed that when I got near the end of the food, way past full but still eating, I was in such a state that I was acting as if I was completely compelled. I was rushing. I was working hard. I was in a state of pressure. It was like being in an eating marathon with me as the only contestant -- but I was completely and devastatingly in earnest. When I noticed this, I allowed me to relax, to breathe, and come down. Dont know what to say about that for anyone else -- but for me that was a discovery.
I am praying and asking God to guide me on this one. I want to conquer it and know I need His help. Thank you Lord, I know you will show me the way out of this.
Be back soon
--Marcia
I just got back from visiting a friend who had been in a car accident last Wednesday. She called and told me about it on Saturday and hearing about it felt so shocking to me. I am so glad she was not injured more than she has had to deal with. Her leg is hurting her and her neck and shoulders, too. I took a little food and she and her two grand daughters and I had dinner together and talked and shared. I am so grateful to God that He spared her life this time. It really shows you just how precious life is and that we have only been granted so much time on Earth. That being true, puts things into a whole different perspective. God, family, and friends become so much more important.
I have been listening to "The Great Health Debate" which was eight days of one-hour health interviews of at least 16 different healthy living teachers covering the spectrum from vegan, meaning eating no meat or animal products of any kind, to the polar opposite which is those who eat meat for health. Wow. I have got to tell you this was really amazing to me to listen to such informed people and to find out why they do what they do. The most important thing to come from it all is this: what am I going to do with this information? We are all in that boat. What are you going to do in your life with the information you have.
Sean Croxton ( www.undergroundwellness.com ) one of todays experts said: "We are all different. We have something called biochemical individuality. The thing that works for me, may not work for the next person. Just eat real food. What I teach people is to listen to their body "language." Do what works for you." He also said, again, "Just eat real foods. Just eat foods that came out of the ground, eat foods that came (from) animals. Get rid of all the processed junk. Get rid of all the "new" foods. Be very wary of grains and legumes, and dairy products as well -- for a lot of people -- because of what they may do to the gut and the anti-nutrient properties that they can have. I try to keep it really simple for people so I tell them to eat real food." He also described going with the starting place of half of your plate animal food and the other half primarily vegetables. Once you try that then make the adjustments that your body tells you to make.
He talked about keeping it old school -- eating the same meat, fish, vegetables that we have eaten forever. He said that he does not believe that an old food will cause a new disease. Makes sense to me. He talked about our human genes having been around for thousands and thousands of years and there is food out there that has not been around for even twenty years. Shy away from that stuff. Keep it simple (without a lot of sauces and exotic concoctions). Keep it real (actual food, not chemically altered). Get rid of the processed food (manufactured food stuff) and eat real food. I am still going to cook my meat but the veggies should be raw. And I would add for us diabetics to get rid of all sugars. You can get along without them. High blood sugar comes from eating sugar and things that turn into sugar in the gut (grains, starchy foods, starchy vegetables).
Sean also quoted this statement: "Anything worth doing is worth doing poorly at first." It is an odd statement but there is some truth in it. I chuckled when he said it because I felt like I knew exactly what he was talking about. You cannot change your whole diet and be successful in just one day, it takes practice, it takes trial and error -- and if you are willing to start off doing it poorly, then you will continue until you do it better -- or you find a better way to do it. Who knows, one day you could end up being an "expert" but no one starts out there. Sometimes people are not willing to do things poorly, but in reality that is where every one is when you start. No one is perfect, even when they get to be experts, there is always something to work on.
After listening this week to the debate airings I am feeling relieved. I had been feeling down and discouraged because I just do not seem to be able to stick to a vegan diet, which I had felt was the right thing to do for my health. I felt that my "giving in" and starting to eat meat again was somehow a failure on my part, but the truth is, to fail means to quit and I have not quit, I am just continually making adjustments. I have had to change my mind and approach often, to keep up with the reality of my own life. Who is to say that being a vegan is the right thing for me to do? It works for some, but it surely wont work if you cannot stay on it.
I think it all boils down to mindful eating which Mike Adams ( http://www.naturalnews.com/index.html ) talked about. He talked about simply paying attention to what you are eating and thinking about it. He pointed out that most American and Europeans eat "mindlessly" -- using that word as a technical term meaning eating without thinking about what you are eating.
I know for myself, when I am eating things that I want to eat but know will harm my body in some way I have to turn off what my mind is saying about it. That is mindless eating. That is responding to feelings of some kind without responding to health or consequences.
For me, mindful eating would be choosing lots of fresh raw vegetables and also choosing healthy meat to eat. The thing is... that is what the Lord told me a long time ago. I have known that is the best solution for me all along, but, if not for the "30 Day Diabetes Cure" by Dr Ripich and Jim Healthy, I would not have started the journey to get close to my own ideal.
I know that I need to stay away from all sugars, including artificial or "new" sugars, like xylitol. It was trial and error that revealed the problems for my body with eating xylitol. I tried it. I erred. I corrected. I no longer eat that. I know that I should avoid all grains, too, but what I actually do is limit them. I do eat some food, occasionally, that is made from grain or flour. The ideal is "never" -- the practical ideal is "rarely." But even that is not where I live. Where I have a problem is with this "mindless" eating thing. Eating as if I have no mind. Purposefully making wrong choices for myself.... out of habit.... out of desire... out of some compulsion that I have. I would love to learn how to conquer that!!
This is a personal journey of discovery. As I was assembling my trash for disposal today the empty cracker boxes from last Wednesday when I bought some "healthy" crackers and ate them with either cottage cheese or avocado dip came rushing back into my consciousness. I also remembered the stomach cramps I got after having eaten them. The empty pizza box from Sat night slapped my face with remembrance, too. It is the mindless eating that I want to conquer. Looking for a solution to that.
I have noticed something about the mindless eating episodes that I had not noticed before. When I am doing that, there is a pressure inside of me. The last couple of times I did that, I noticed that when I got near the end of the food, way past full but still eating, I was in such a state that I was acting as if I was completely compelled. I was rushing. I was working hard. I was in a state of pressure. It was like being in an eating marathon with me as the only contestant -- but I was completely and devastatingly in earnest. When I noticed this, I allowed me to relax, to breathe, and come down. Dont know what to say about that for anyone else -- but for me that was a discovery.
I am praying and asking God to guide me on this one. I want to conquer it and know I need His help. Thank you Lord, I know you will show me the way out of this.
Be back soon
--Marcia
The Institute of Medicine and the Inconvenient Truth of the Real Affordability of the Affordable Care Act
Tuesday, January 28, 2014
 Enshrining a term only an actuary could love, the Affordable Care Act sets health insurance coverage on the basis of "actuarial value" (AV). A good summary can be found in this Consumers Union Health Policy Brief. As the Disease Management Care Blog understands it, AV is the percent of typical medical expenses that a health insurance policy will cover for a typical population. In other words, some individuals will have no out of pocket expenses (deductibles, coinsurance and limits) while other individuals will have end up paying for most of their services. When those expenses are rolled up over thousands of persons and compared to total health care costs, the percent left over is the "AV."
Enshrining a term only an actuary could love, the Affordable Care Act sets health insurance coverage on the basis of "actuarial value" (AV). A good summary can be found in this Consumers Union Health Policy Brief. As the Disease Management Care Blog understands it, AV is the percent of typical medical expenses that a health insurance policy will cover for a typical population. In other words, some individuals will have no out of pocket expenses (deductibles, coinsurance and limits) while other individuals will have end up paying for most of their services. When those expenses are rolled up over thousands of persons and compared to total health care costs, the percent left over is the "AV."Once the Disease Management Care Blog wrapped its head around the AV, it next tackled the ACA concept of the "essential health benefit" (EHB). This is the minimum package of covered services (outpatient, emergency room, maternity, hospitalization, medications, rehabilitation and the like) that a health insurer must include in its coverage plan. This will ultimately be defined in yet-to-be-determined federal regulations.
Now that we have the jargon nailed down, plans that fail to meet at least 60% of AV on the EHB will be excluded from the exchanges and ineligible for federal subsidies. 60% is "bronze" coverage, while 70%, 80% and 90% are "silver," "gold" and "platinum," respectively. This is important because not only did most members of Congress not understand AV (consumer costs) or EHB (coverage), but because both will determine the future cost of our nations health care bill.
Enter the Institute of Medicine (IOM), which has just released a report on how the Feds should best determine the EHB. A handy summary can be found here.
Bottom line?
The IOM has backed into the EHB, not basing it on notions of optimum health coverage but on affordability. It recommends that the basic affordable EHB be based on a survey of what is typically covered by an insurance plan that is purchased by a small business employer. With that as the baseline, the EHB be further modified (based on scientific evidence and public input) so that the premium ultimately matches 70% of the small business AV. According to John Iglehart writing in the New England Journal of Medicine, that could work out to be about $5000 per year for individuals and about $13,500 for families.
This is significant because the key underlying assumption of the ACA was that forcing everyone in the risk pool (with the Constitutionally suspect "play or pay" provision) with insurance rich in wellness, prevention and services like rehab, mental health and pediatric oral care would, by itself, drive down health costs.
The smart folks over at the Institute of Medicine respectfully disagree. They believe the best approach is to figure out what is affordable first and then define the insurance coverage second.
Its finally happened. While its not explicitly stated, the Federal deficit has noisily bumped into the Affordable Care Act. The IOM has given the ACAs supporters cover over the inconvenient intrusion of costs into coverage, affordability into access and reality into fantasy. Even if the IOM recommendations fall on deaf ears, DMCB readers can expect the the Federal budgets problems to now and forever be part and parcel of the ACA.
What to do? When the Disease Management Care Blog is flummoxed, it likes to break into song. One song that comes to mind is Taxman......
Subscribe to:
Posts (Atom)





