Showing posts with label u. Show all posts
Showing posts with label u. Show all posts
U S Public Schools and the First Line of Defense in the Early Detection and Treatment of Mental Illness
Tuesday, April 15, 2014
 What the Disease Management Care Blog didnt quite appreciate was the potential role of the U.S. public school system in helping people like "Tim."
What the Disease Management Care Blog didnt quite appreciate was the potential role of the U.S. public school system in helping people like "Tim." It thought the fundamental purpose of teachers was to teach. Yet, when it considers that the hours that a child spends in school is an opportunity to catch problems that may be missed by parents and docs alike, the idea that schools can be a first line of defense in the early detection of mental illness has some merit.
For your consideration when youre grappling with your local school taxes:
Tim is the son of Paul Gionfriddo, who is a former Connecticut politician and current mental health advocate. As the parent of a child with schizophrenia, he knows what hes writing about.
When Mr. Gionfriddo was starting out as a legislator, he was only just becoming aware of Tims difficulties in school. What followed was heartbreaking tale of inflexible school officials arranging for the wrong evaluations, wrong diagnoses, inadequate care and wasted attempts to help a deeply troubled child. Teachers were unable to cope, the parents were often blamed and Tim got shuffled around an unresponsive school system. Despite "good" insurance, coverage fell short and many services involved onerous co-pays and limitations. And once he reached adulthood, an unwillingness to accept services moved Tim to the margins of society, leading to repeated hospitalizations and incarcerations. He now lives in squalor somewhere in San Francisco.
Tims story is not unique. According to Mr. Gionfriddo, a well meaning policy that moved hundreds of thousands of mentally ill out of decaying inpatient psychiatric hospitals in the 1980s was followed by
1) schools being unable to handle children with mental illness,
2) underfunding of community agencies, and
3) the siloing of the resources that did exist, resulting in little collaboration among physicians, law enforcement, community services or the mental health community.
Among Mr. Gionfriddos recommendations? In addition to better screening by pediatricians during the well child visit, insurance orm and better housing options, state legislators should support the following:
1. The U.S. public school system should be prepared to offer mental health services in addition to basic education;
2. Every teacher should receive training in recognizing mental illness and how to handle it;
4. Once mental illness is discovered, meaningful support should be included in a childs individualized education planning.
Image from Wikipedia

Health Care Reform in the U S vs Other Developed Countries
 |
| Your doctor will see you now! |
Victor Fuchs, writing in the Jan 2 edition of JAMA, has a slightly different perspective. He notes that American history is dominated by waves of immigrants who came here to escape oppression. We are far more distrustful of government. We are also less likely to support redistributive public policies. That may be partly due to a more heterogeneous population that is less sympathetic to the less fortunate when they fall outside the right social or demographic class. Last but not least, our system of government is quite inefficient compared, say, to a parliamentary system.
Thats why:
1. Government spending on health care is comparatively lower: 46% in the U.S. vs. 75% in Organization for Economic Co-operation and Development (OECD) countries. As a result, a) administrative costs are fragmented, and b) there is less ability to negotiate prices with providers and suppliers
2. There is a different mix of services: in the U.S., less top-down control means more high tech, specialists and amenities with relatively less reliance on physicians and hospitals to render health care services.
What is the way forward? Dr. Fuchs recommends that future health orm efforts not be modeled on Europe. Instead, Americans should scale back their expectations and focus on what is necessary, not desireable.
If government is to assume a greater share of health care costs beyond the current 46% level, it should probably worry about funding basic care, not all care. In addition, Americans are less likely to support total equality; they want to preserve the option of "buying up" when they can afford it. Last but not least, future orm is going to have to find a middle ground between all the advocacy groups, stakeholders and special interests that dominate the mix of services.
Image from Wikipedia
U S Government Launches a Population Health Improvement Initiative Called Million Hearts
Thursday, February 27, 2014
 The Department of Health and Human Services (HHS) has launched a "Million Hearts" campaign that is designed to prevent a million heart attacks and strokes in the next 5 years. You can read about it in the New England Journal here or in Circulation here. There is also more detail here at the HHS gov web site.
The Department of Health and Human Services (HHS) has launched a "Million Hearts" campaign that is designed to prevent a million heart attacks and strokes in the next 5 years. You can read about it in the New England Journal here or in Circulation here. There is also more detail here at the HHS gov web site.The campaign is crafted to address the "ABCS" a.k.a. aspirin, blood pressure control, cholesterol control and smoking in the U.S. population. The Feds propose to 1) consolidate just how ABCS will be specifically measured in any population, 2) remind and help manufacturers as well as users of EHRs that they can be tasked to addressing ABCS, 3) initiate a "pharmacist-led campaign.... (to) facilitate counseling about hypertension control," 4) launch an anti-tobacco marketing and community-based campaign, 5) push for food labeling in restaurants and 6) increase the measurement of sodium and fat consumption. Details are in this table.
"Bravo!" says the DMCB. When it reads about Million Hearts, its clear that the Feds are identifying population-based strategies, basing their interventions on demonstrated needs, increasing awareness of health risks, using patient-friendly education, helping consumers make the right choices and figuring out how to assess outcomes on an ongoing basis with a feedback loop.
If you agree on the DMCBs assessment of what the Feds are up to, you also agree that theyve they have launched a huge population health improvement (PHI) initiative. The DMCB isnt making that up: if you compare the Care Continuum Alliance description of PHI here with the fundamentals of Million Hearts, youll see that the overlap is almost 100%.
Whats different is that the Feds are also using Million Hearts to 1) further justify the Affordable Care Act and the EHR meaningful use initiative, 2) leverage some potent government entities like AHRQ, CDC, CMS and the FDA, 3) distribute hundreds of millions in community grant money, 4) create a coalition that includes The Y, AHA, Walgreens, some professional pharmacy associations and AHIP, and 5) say some nice stuff about Mrs. Obamas childhood obesity program.
All that makes perfect sense from a governmental as well as political process, but its still PHI.
"A hearty welcome to the fold!" says the DMCB. HHS has finally decided to give millions of Americans access to PHI that combats atherosclerotic heart disease. Better late than never, but based on what we know about the science of PHI in multiple other settings and assuming the government can pull this off, the DMCB is confident that a million lives being saved is within reach.
Real News Headline Improved U S Health Care System Saves 28 000 Lives in 2010 Avoidable Death Rate is Decreasing
Sunday, February 9, 2014
.jpg) |
| Health reporters at work |
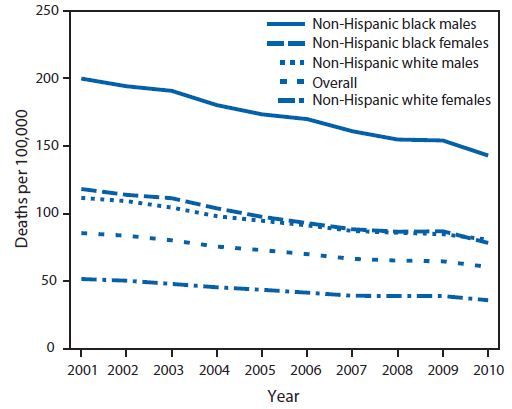
The information reported in the media was taken from the Centers for Disease Control and Preventions Sept. 3 Morbidity and Mortality Weekly Report. As the DMCB understands it, the CDC authors pulled 2001-2010 mortality data from the National Vital Statistics System. Once that was done, they counted up the number of persons aged less than 75 years who died of "ischemic heart disease," "cerebrovascular disease," hypertensive disease" or "chronic rheumatic heart disease."
So what did MMWR really say?
The total of "less-than-75" deaths in 2001 was 227,961. For 2010, it was lower at 200,070. Since the population in the U.S. has changed over the last decade, the totals for each of the two comparison years were then expressed as a "per 100,000" statistic.
Since 2001, the "less-than-75" death rate per 100,000 declined by 29%. The decline averaged 3.8% a year.* Persons age 65-74 years had an average decline of 5.1% vs. 3.3% persons between the ages of 55-64.
The good news is that Black (3.9%) and Hispanic (4.5%) persons had greater declines than whites (3.6%). The bad news is that they started and ended with a higher death rate.
Heres a visual display of the data:
The DMCBs take
1. "Avoidable?" The CDC definition implies that perfect control of all cardiac risk factors (for example, cholesterol and weight) for everyone under the age of 75 will result in a 0 per 100,000 cardiovascular death rate. Not so, because those risk classic factors capture some, but not all, persons who succumb to heart attack and stroke.
2. So, this is bad news? "200,000" deaths is an impressive number, but, on an unadjusted basis, thats about 28,000 fewer compared to 10 years ago. Some additional good news is that the U.S. rate of non-fatal heart attack and stroke appears to have dropped significantly also. We are making significant headway in the battle against heart disease.
3. The real story? Persons of color have had the greatest relative benefit but still have the greatest absolute need. That lingering health care disparity went shamefully unmentioned by CNN and was only briefly mentioned by USAToday.
4. Something for everyone: In their "Conclusions and Comments," the authors of the MMWR paper speculated on the benefits of the (still unproven) Million Hearts Initiative (a Berwick-era idea) as well as "health information technology" and various "community prevention strategies" The DMCBs colleagues in the care management service industry will really like the authors nods toward "team based care" and how "individuals can work toward reducing their own heart disease and stroke risk." If the CDC says so, it must be true - assuming theres a good business model.
5. Speaking of speculation, the authors wondered if the greater decline in the Medicare age group (65-74 years) versus the younger age group (55-64) was because of the presence of health insurance. Maybe, but maybe not. The DMCB also wonders if heart disease is more lethal and less amenable to intervention among younger persons, but cant find any literature to back that up.
6. Politics intrude: Naturally, the scientists who write MMWR are too classy than to curry favor with the appointees that populate the upper echelons of the federal bureaucracy, but that didnt stop the CDC Vital Signs from shamefully putting in a "making it easier for Americans to afford regular preventive health care through the Affordable Care Act" plug. The ACA was not mentioned in the MMWR report because the declines mentioned above occurred in the absence of the ACA.
The DMCB predicts that when the "avoidable" death rate continues to decline by 3.8% in the coming years, Obamacare advocates will take the credit.
*The DMCB isnt sure how 3.8% for 10 years makes for 29% either, but thats statistics for you.
Image from Wikipedia
An HBO Newsroom Inspired Rant Over the U S Health Care System
Sunday, January 26, 2014
If you are distressed by the United States decline, doubt American exceptionalism, share in the angst infecting the progressivist salons and enjoy Aaron Sorkins tightly written diatribes, youre probably already aware of (or even forwarded an email link to) this angry rant by the lead Jeff Daniels character in the HBO series "The Newsroom."
Unable to resist, the inspired Disease Management Care Blog tapped Xtranormal to imagine a Newsroom-esque angry rant over the widely accepted notion that U.S. health care is so awfully broken.
References:
The Commonwealth Fund: Explaining High Health Care Spending in the United States: An International Comparison of Supply, Utilization, Prices, and Quality
OECD: Why Is Health Spending in the U.S. So High?
OECD: Health At A Glance 2011 OECD Indicators
University of Pennsylvania Scholarly Commons: Low Life Expectancy in the United States: Is the Health Care System at Fault?
U.S. Newborn Rate Tied with Qatar? Not Exactly.
CODA: The DMCB also rises to second the Fat Ladys probable belief that, despite Newsroom character Wills disdain, angels do exist.
Unable to resist, the inspired Disease Management Care Blog tapped Xtranormal to imagine a Newsroom-esque angry rant over the widely accepted notion that U.S. health care is so awfully broken.
References:
The Commonwealth Fund: Explaining High Health Care Spending in the United States: An International Comparison of Supply, Utilization, Prices, and Quality
OECD: Why Is Health Spending in the U.S. So High?
OECD: Health At A Glance 2011 OECD Indicators
University of Pennsylvania Scholarly Commons: Low Life Expectancy in the United States: Is the Health Care System at Fault?
U.S. Newborn Rate Tied with Qatar? Not Exactly.
CODA: The DMCB also rises to second the Fat Ladys probable belief that, despite Newsroom character Wills disdain, angels do exist.
Subscribe to:
Posts (Atom)





